
That searing pain shooting from your lower back down your leg can derail your life. When stretches and painkillers fall short, your doctor might suggest an epidural for back pain—a precision treatment delivering anti-inflammatory medication directly to the nerve roots causing your agony. Unlike epidural anesthesia used in childbirth, this procedure targets inflammation without numbing your entire body. You’ll discover exactly when it’s recommended, what happens during the injection, realistic recovery timelines, and how to maximize your results. Most importantly, you’ll learn why this treatment creates a crucial window for rehabilitation when other options fail.
Why Your Nerves Need Targeted Steroid Relief
A lumbar epidural steroid injection places corticosteroid medication into the epidural space—the protective sleeve surrounding your spinal nerves. This space contains nerves, blood vessels, and connective tissue. When nerve roots become compressed or inflamed from conditions like herniated disks, the steroid reduces swelling and pressure at the exact source of your pain. This breaks the vicious cycle where pain causes muscle spasms, which then create more pain.
How Steroids Shut Down Nerve Inflammation
Corticosteroids work by suppressing your body’s inflammatory response around irritated spinal nerves. As swelling decreases, pressure on nerve roots eases, reducing both localized back pain and radiating leg symptoms. Crucially, relief isn’t immediate—it typically takes 2-7 days for the medication to reach full effectiveness. During this period, you might experience temporary pain fluctuations as your body responds to the treatment.
Conditions That Warrant an Epidural for Back Pain
Doctors reserve epidural injections for cases where physical therapy, medications, or lifestyle changes haven’t provided sufficient relief. The strongest evidence supports their use for:
- Sciatica (lumbar radiculopathy): Sharp, shooting pain traveling from your low back through your buttock and down your leg
- Herniated lumbar disks: When disk material directly presses on nerve roots
- Lumbar spinal stenosis: Narrowing of the spinal canal compressing nerves during standing or walking
- Neurogenic claudication: Leg pain triggered by activity and relieved by sitting
Proven insight: Patients with acute radiculopathy (recent onset) typically see better results than those with chronic pain lasting over six months. If your MRI confirms nerve root compression matching your symptoms, you’re an ideal candidate.
Your Epidural for Back Pain Procedure: Step-by-Step
The Specialists Performing Your Injection
Board-certified physicians with advanced spine training handle your epidural for back pain, including:
– Physiatrists (Physical Medicine & Rehabilitation specialists)
– Interventional anesthesiologists
– Spine-trained radiologists or surgeons
All use real-time imaging guidance to ensure precision—never blind needle placement.
Critical Pre-Procedure Steps You Must Complete
Don’t skip these preparation essentials:
– Bring imaging reports: Provide recent lumbar X-rays, MRI, or CT scans showing your problem area
– Disclose all substances: List every medication, supplement, and herbal product (even fish oil)
– Arrange transportation: Required if receiving sedation (common for anxiety)
– Verify pregnancy status: Inform staff if pregnant—fluoroscopy uses minimal radiation
Skipping these steps could delay your procedure or create safety risks.
What Happens During the 15-Minute Injection
- Positioning: You’ll lie face-down on a padded table
- Sterile setup: Back cleaned with iodine and covered with surgical drapes
- Numbing: Brief sting as lidocaine anesthetizes the skin
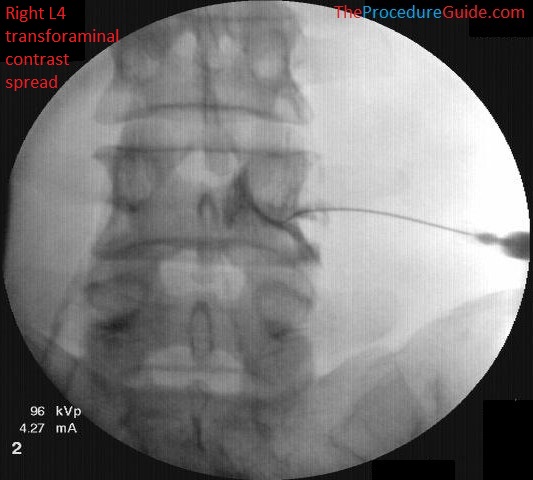
- Guided needle placement: Using live X-ray (fluoroscopy), the doctor advances a thin needle to your epidural space
- Dye confirmation: Contrast dye verifies correct placement before medication
- Steroid delivery: Corticosteroid (sometimes mixed with local anesthetic) flows slowly
- Monitoring: Brief observation for immediate reactions
Realistic Sensations During Treatment
Expect these normal experiences:
– Sharp pinch during skin numbing (lasts seconds)
– Pressure or warmth as medication spreads
– Brief reproduction of your pain if the needle nears an irritated nerve (resolves quickly)
– No electric shocks—unlike nerve conduction tests
Your doctor will communicate throughout, stopping if you feel unusual pain.
Recovery Timeline: What to Expect Hour-by-Hour
First 24 Hours After Your Epidural
- Discharge: Leave within 30 minutes if no sedation issues
- Activity: Rest completely for the remainder of the day
- Soreness: Ice the injection site for 15 minutes hourly to reduce tenderness
- Driving restriction: Avoid operating vehicles for 24 hours if sedated
Critical note: Do not resume physical therapy exercises until cleared by your provider—usually 48 hours post-injection.
Managing the 72-Hour Pain Flare
Up to 30% of patients experience temporary pain worsening for 2-3 days as the steroid crystallizes before dissolving. This isn’t treatment failure—it’s a normal precursor to relief. Combat it with:
– Ice packs (15 minutes on, 1 hour off)
– Walking short distances hourly
– Prescribed pain medication (avoid NSAIDs initially if instructed)
When Relief Actually Starts—and How Long It Lasts
- Day 2-7: Gradual pain reduction begins
- Weeks 2-4: Peak effectiveness for most patients
- Duration: 3 weeks to 6 months for 70% of herniation patients
- Long-term: 40% maintain ≥50% pain reduction at 12 months
Realistic expectation: This isn’t a cure—it buys time for rehabilitation. One study showed patients achieving significant relief were 3x more likely to avoid surgery within two years.
Potential Side Effects: Separating Normal From Dangerous
Common Temporary Reactions (Last 1-3 Days)
- Increased back/leg pain
- Headache or dizziness
- Facial flushing or warmth
- Sleep disturbances
- Nausea
These resolve without intervention and shouldn’t deter you from follow-up treatments if needed.
Serious Complications Requiring ER Care
Seek immediate help for:
– Severe headache that vanishes when lying flat (dural puncture)
– New weakness or numbness in legs
– Loss of bowel/bladder control
– Fever over 100.4°F or spreading redness at injection site
– Unrelenting back pain worse than pre-procedure
While permanent nerve damage occurs in fewer than 1 in 10,000 injections, recognizing these red flags prevents complications.
Maximizing Your Pain Relief Results

Why You’re Limited to 2-3 Injections Yearly
Most clinics enforce strict 2-3 epidural for back pain limits annually due to:
– Cumulative steroid exposure risks (bone weakening, adrenal suppression)
– Diminishing returns after multiple injections
– Potential masking of progressive structural issues
Exceeding this increases osteoporosis risk without improving outcomes.
The Rehabilitation Partnership That Makes It Stick
Your epidural for back pain only creates a pain-free window—it won’t fix underlying problems alone. For lasting results:
– Start physical therapy within 72 hours of relief onset
– Perform prescribed core-strengthening exercises daily
– Maintain ergonomic modifications at work/home
– Follow activity pacing (e.g., walk 10 minutes hourly)
Patients combining injections with structured rehab achieve 50% greater long-term pain reduction than those relying solely on injections.
When to Call Your Doctor Immediately After Treatment
Don’t wait if you experience:
– Leg weakness making stairs difficult
– Numbness in saddle area (inner thighs/buttocks)
– Fever with chills within 72 hours
– Headache requiring lying flat to function
– Uncontrolled pain despite rest and ice
These signal potential complications needing same-day evaluation.
Long-Term Management After Epidural Success
Realistic outcomes vary significantly—some get minimal relief while others enjoy months of freedom from pain. The critical factor is using the pain-free period to build strength. Epidural for back pain treats inflammation but doesn’t repair herniated disks or reverse spinal stenosis. Patients who commit to core stabilization exercises after injections reduce recurrence risk by 60% compared to passive treatment approaches. If relief fades before rehabilitation goals are met, discuss alternative options like radiofrequency ablation rather than additional steroids.
Your Action Plan for Epidural for Back Pain Success
- Allow 7 days before judging effectiveness—don’t confuse pain flare with failure
- Resume walking within 24 hours (start with 5-minute intervals)
- Track pain levels daily using a 0-10 scale
- Communicate new symptoms immediately to your provider
- Prioritize physical therapy over pain medication during relief periods
Back pain affects 1 in 4 adults annually, making epidural for back pain one of North America’s most common interventional procedures. When used strategically within a comprehensive plan, it provides the critical pain relief needed to rebuild strength and reclaim your active life—without rushing into surgery. Remember: its greatest power lies not in masking pain, but in creating the opportunity for lasting recovery through movement.