
That sharp twinge when you bend to tie your shoes. The dull ache that won’t quit after sitting at your desk. Back pain strikes without warning—one moment you’re functioning normally, the next you’re modifying every movement to avoid discomfort. Your spine, that remarkable column of 33 vertebrae supporting your entire body, suddenly feels like it’s working against you. Whether it’s cervical spine pain radiating into your neck or lumbar spine discomfort shooting down your leg, spinal pain affects 80% of adults and can transform simple daily tasks into major challenges.
The good news? Most spine-related back pain responds to targeted treatments and prevention strategies. This guide walks you through understanding your specific spinal condition, identifying the exact source of your discomfort, and accessing proven solutions—from conservative therapies to cutting-edge treatments. You’ll learn how to decode your symptoms, navigate diagnostic options, and implement effective interventions that address the root cause rather than just masking the pain.
Pinpoint Your Exact Spinal Pain Source
Cervical, Thoracic, or Lumbar: Matching Pain to Spinal Region
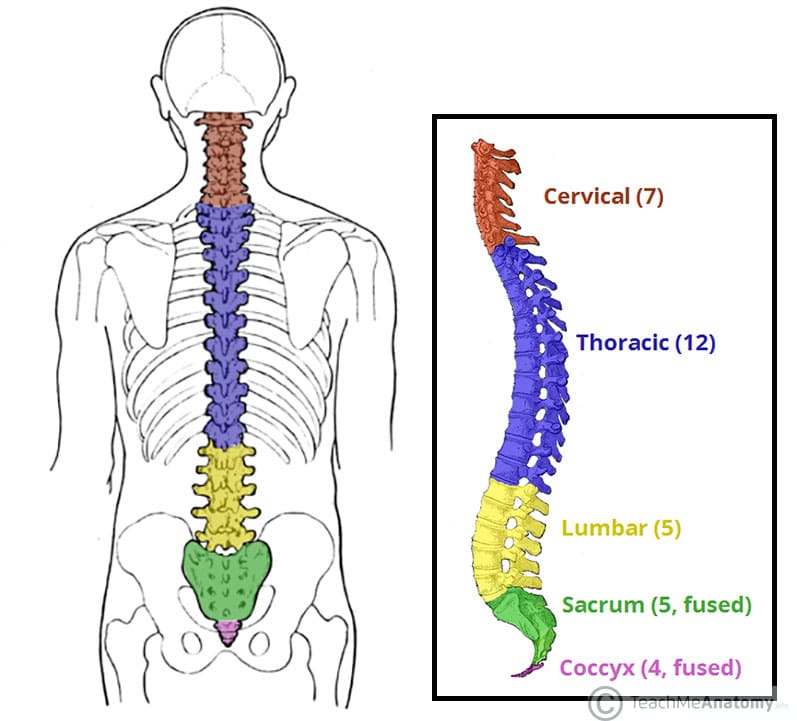
Your spine divides into distinct regions, each with unique pain signatures. Cervical spine pain (C1-C7) radiates into your neck, shoulders, and arms, often causing headaches that worsen with screen time. Thoracic spine discomfort (T1-T12) wraps around your rib cage, potentially mimicking heart or lung problems—many patients initially mistake it for cardiac issues. Lumbar spine pain (L1-L5) concentrates in your lower back, frequently shooting down your legs as sciatica when discs herniate at L4-L5 or L5-S1 levels.
The sacral region (S1-S5) creates pelvic and buttock pain that intensifies when sitting, while coccygeal issues cause tailbone pain when transitioning from standing to sitting. Understanding these regional patterns helps you and your healthcare provider pinpoint the exact source of your discomfort rather than treating back pain generically.
Disc Damage vs. Nerve Compression: Identifying Your Pain Mechanism
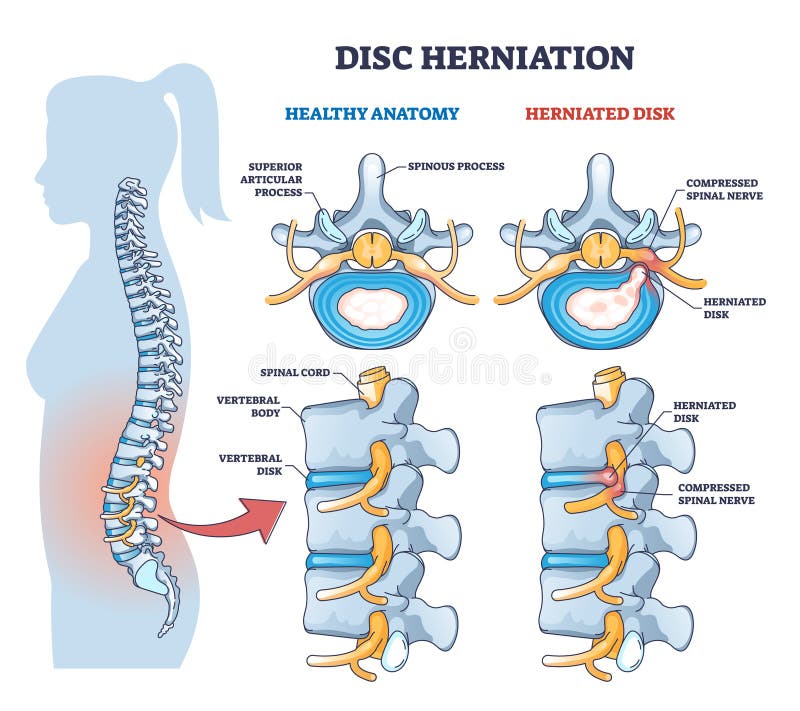
Between each vertebra, intervertebral discs act as shock absorbers with a tough outer layer surrounding a gel-like core. When these discs herniate, the inner gel pushes through outer tears, potentially compressing spinal nerves and creating sharp, shooting pain along affected nerve pathways. Degenerative disc disease—a natural aging process—causes chronic mechanical pain that worsens with activity and improves with rest.
Spinal stenosis creates a distinctive symptom pattern: leg pain and weakness triggered by walking that improves immediately when you sit or bend forward. This “neurogenic claudication” differs from vascular claudication (caused by poor circulation), which doesn’t improve with forward bending. Pro tip: If walking 300-500 feet triggers leg pain that forces you to stop, but sitting on a bench provides relief within minutes, spinal stenosis is likely your culprit.
Decode Your Symptoms Before Seeking Treatment
Emergency Warning Signs Requiring Immediate Care
Certain symptoms demand same-day medical attention. Progressive leg weakness, loss of bladder/bowel control, or numbness in the saddle area could indicate cauda equina syndrome—a surgical emergency requiring treatment within 24-48 hours to prevent permanent damage. Fever, unexplained weight loss, or pain that worsens at night might signal infection or tumors rather than mechanical back pain.
Red flag checklist: If your back pain follows significant trauma like a fall or car accident, seek evaluation even if symptoms seem mild. Spinal fractures aren’t always obvious initially but can worsen without proper treatment. Night pain that wakes you from sleep—especially without positional relief—warrants prompt investigation.
Movement-Based Pain Assessment You Can Do at Home
Your pain’s relationship to movement provides crucial diagnostic clues. Disc-related pain typically worsens with forward bending, sitting, or lifting. Try this test: Lie on your back and pull one knee toward your chest. If this relieves your pain, a herniated disc is likely. If it worsens your pain, facet joint arthritis may be the culprit.
Facet joint pain increases with extension and rotation—notice if leaning backward or twisting your torso intensifies discomfort. Spinal stenosis creates the “shopping cart sign”—you’ll find relief by leaning on shopping carts or walkers while walking. Document these movement patterns before your doctor’s visit to help target your diagnosis.
Maximize Conservative Treatments Before Considering Surgery
Physical Therapy Protocols That Deliver Real Results
Physical therapy forms the backbone of non-surgical spine treatment, but not all exercises work for every condition. For disc herniation: Start with McKenzie extension exercises—lying face down with elbows under shoulders, gradually increasing extension time. Perform 10 repetitions hourly during acute pain.
For spinal stenosis: Focus on flexion-based exercises like knee-to-chest stretches and pelvic tilts. Core strengthening should target deep abdominal muscles (transverse abdominis) through modified planks and dead bugs, not traditional sit-ups that strain the spine. Pro tip: Hold each core exercise for 5-10 seconds initially, working up to 30 seconds as strength improves—quality matters more than quantity.
Medication Strategies with Clear Dosing Guidelines
NSAIDs like ibuprofen work best at maximum doses initially (800mg three times daily for 3-5 days), then taper to lowest effective dose. Never exceed 2400mg daily due to gastrointestinal and cardiovascular risks. Muscle relaxants like cyclobenzaprine (5-10mg three times daily) should be limited to 7-14 days due to sedation risks—never combine with alcohol.
For nerve-related pain, gabapentin starts at 300mg at bedtime, increasing by 300mg every 3-4 days as tolerated up to 1800-3600mg daily. Pregabalin begins at 75mg twice daily, potentially increasing to 300mg twice daily. These medications require gradual titration to minimize dizziness and drowsiness.
Prevent Future Episodes With Targeted Strategies
Ergonomic Modifications That Actually Work
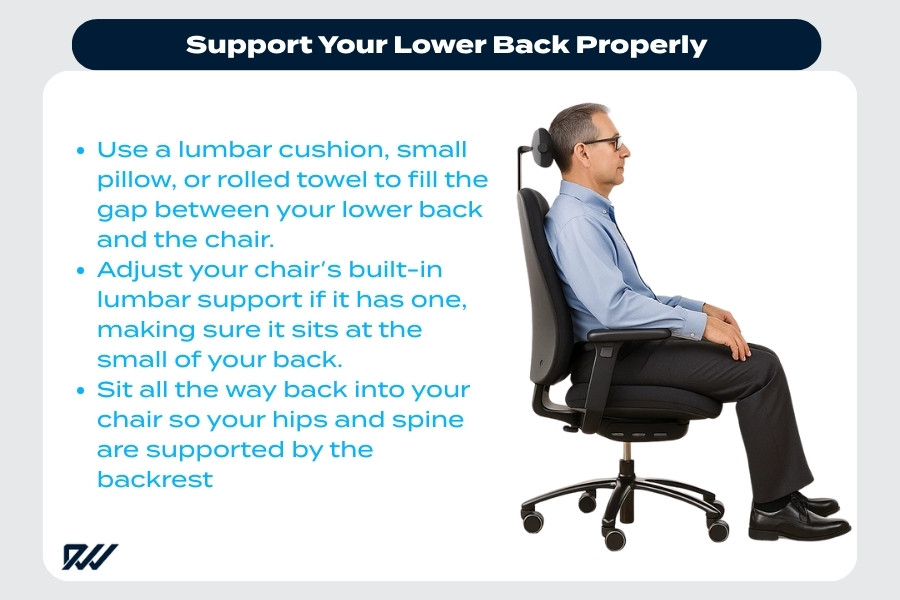
Workstation setup requires specific measurements: Position monitors so the top third aligns with your eye level, keeping your neck in neutral alignment. Your keyboard should sit at elbow height with shoulders relaxed—use a footrest if feet don’t rest flat. Lifting techniques must be practiced: Stand within 6 inches of the object, bend knees (not waist), keep the load close to your body, and avoid twisting while moving.
Sleep posture needs personalized solutions: Back sleepers require a pillow under knees; side sleepers need a pillow between knees maintaining hip alignment. Pro tip: Place a rolled towel in the small of your back while sitting to maintain natural lumbar curve—this simple fix reduces disc pressure by 40% compared to slouching.
Exercise Prescription Based on Your Spinal Condition
Low-impact activities should match your specific condition: Swimming benefits spinal stenosis sufferers, while walking suits most disc-related pain. Strength training frequency matters—perform core exercises every other day to allow muscle recovery. Flexibility exercises require consistency: Hold each stretch for 30 seconds, repeating 2-3 times daily for noticeable improvement in 4-6 weeks.
The optimal exercise formula: 150 minutes weekly of moderate aerobic activity (brisk walking, cycling) plus 2 strength sessions weekly targeting core, glutes, and back muscles. Critical mistake to avoid: Skipping warm-ups—5 minutes of gentle movement before exercise reduces injury risk by 65%.
Special Considerations for Your Life Stage
Pregnancy-Related Back Pain Solutions That Are Safe

Pregnancy affects 50-70% of women due to hormonal changes (relaxin causing ligament laxity), weight gain adding mechanical stress, and postural shifts. Safe management includes pelvic tilts against a wall (10 repetitions hourly), prenatal yoga modifications avoiding deep twists, and maternity support belts worn from second trimester.
Sleep positioning requires strategic pillow placement: Place one pillow under your head, one between knees, and one supporting your abdomen when side-lying. Warning: Avoid lying flat on your back after 20 weeks—this compresses the vena cava, reducing blood flow to both you and baby.
Elderly Patient Treatment Adjustments
Older adults face unique challenges including osteoporosis increasing fracture risk and multiple medications causing interactions. Conservative approaches should be maximized before considering surgery—physical therapy programs must include fall prevention components. Bone density optimization through calcium, vitamin D, and possibly bisphosphonates becomes crucial before any surgical intervention.
Critical consideration: Pain medication selection must account for kidney and liver function changes—dose adjustments for gabapentin and NSAIDs are often necessary in patients over 65.
Your spine supports you through every movement of daily life—return the favor with informed, targeted care. Most back pain improves significantly with appropriate treatment, but persistent or worsening symptoms deserve professional evaluation. Remember: Early intervention prevents minor issues from becoming major problems, and today’s conservative treatments can prevent tomorrow’s surgical needs. By understanding your specific spinal condition and implementing these targeted solutions, you can reclaim pain-free movement and protect your spine for years to come.