

Hunched over your phone or shifting constantly in your chair? You’re part of a staggering global statistic: chronic low back pain affects over 20% of adults and ranks as the world’s leading cause of disability. While acute episodes often fade within a month, persistent discomfort demands targeted back pain therapy that moves beyond basic stretches. The good news? Evidence shows specific interventions can significantly reduce pain and restore function. This guide cuts through the noise to deliver actionable strategies backed by clinical trials—so you can stop guessing and start healing.
Four Clinically Validated Back Pain Therapies That Work
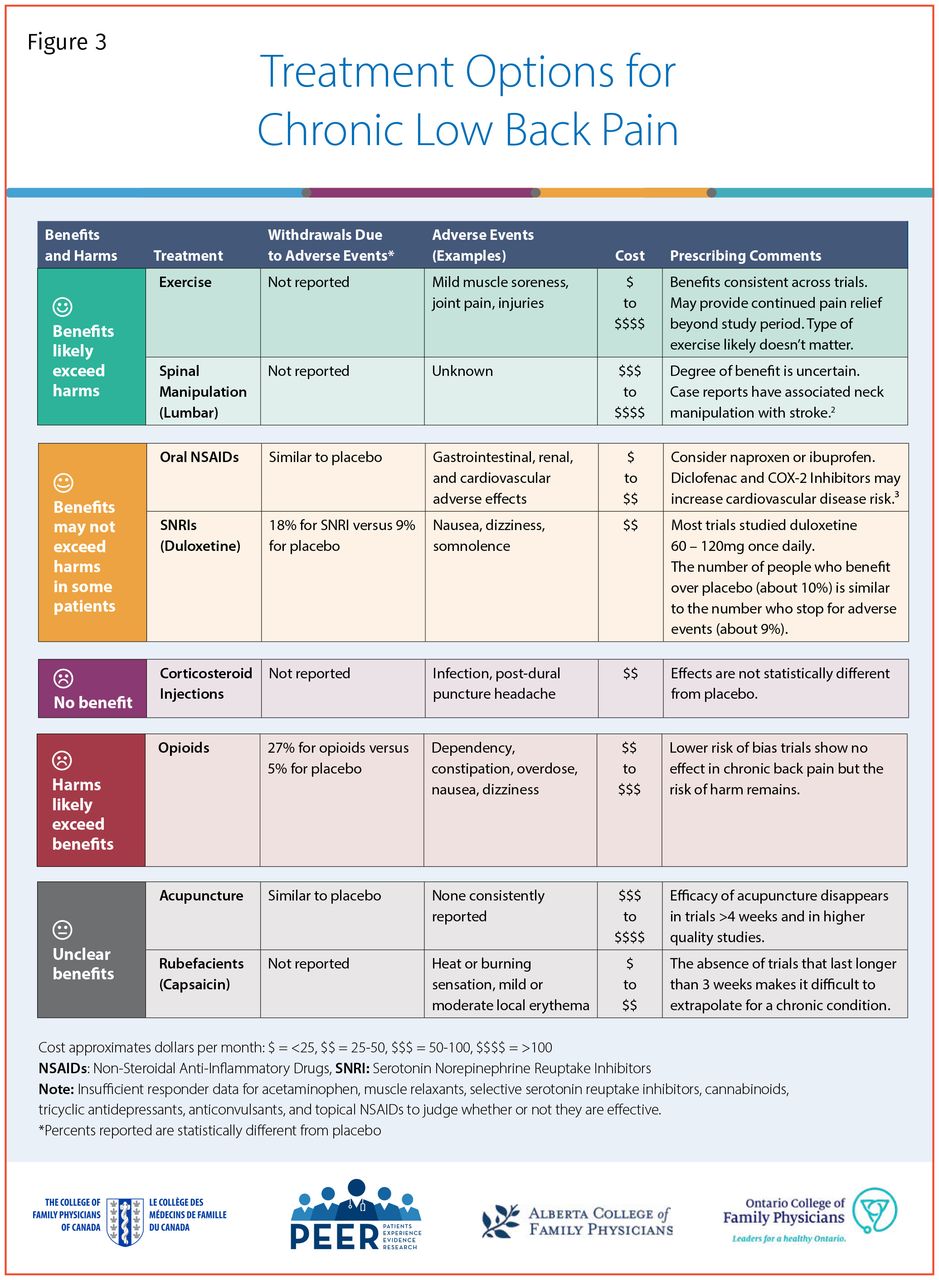
These aren’t temporary fixes but systematically proven approaches with robust evidence for chronic low back pain. Each addresses both pain signals and functional limitations.
How Duloxetine Resets Pain Processing
Duloxetine at 60 mg daily stands as the only medication with high-strength evidence for chronic low back pain. This SNRI works by boosting serotonin and norepinephrine in your spinal cord, effectively dampening pain signals before they reach your brain. You’ll typically notice pain reduction within 1-2 weeks, with benefits deepening over consistent use. While mild nausea or headaches may occur initially, these usually fade within weeks. Crucially, your doctor should monitor for mood changes or rare liver enzyme shifts—especially during the first month—making this back pain therapy ideal when combined with movement strategies.
ACT Therapy: Your Mental Shift for Pain Control
Acceptance and Commitment Therapy (ACT) flips traditional pain management on its head by teaching you to accept discomfort rather than fight it. This high-evidence approach uses mindfulness techniques to build psychological flexibility, helping you focus on valued activities despite pain. Typical programs involve 8-12 sessions with a licensed therapist who guides you through identifying core values and developing action plans. Remarkably, ACT shows superior results for older adults and those with lower education levels—proving you don’t need complex medical jargon to reclaim your life. When paired with physical therapy, it creates a powerful one-two punch against chronic pain cycles.
Precision Exercise Matching: Beyond Generic Stretches
Classification-based exercise protocols use clinical algorithms to match your specific pain patterns with targeted movements. During assessment, your therapist will test directional preferences (like repeated forward bends or side glides) and functional limitations to pinpoint your ideal approach. This method integrates motor control training, manual therapy, and cognitive coaching—delivering large effect sizes for both pain reduction and functional improvement. Unlike one-size-fits-all programs, this back pain therapy systematically addresses why your pain flares during certain activities while ignoring others. Patients with clear directional preferences (like pain easing with backward bends) often see dramatic improvements within weeks.
Digital Programs That Fit Your Schedule
App-based self-management systems deliver structured pain education, movement tutorials, and coping strategies through your smartphone. These moderate-effectiveness tools shine for tech-savvy patients seeking flexible solutions, offering key components like daily pain tracking, progressive exercise libraries, and cognitive-behavioral modules. Guided versions with professional check-ins boost adherence by 30% compared to fully automated apps. While not replacing hands-on care, they provide critical continuity between sessions—especially valuable when in-person therapy access is limited. Look for programs incorporating ODI (Oswestry Disability Index) tracking to objectively measure your progress.
Movement Therapies That Actually Reduce Pain
Exercise remains foundational for back pain therapy, but effectiveness hinges on matching the right movement strategy to your specific presentation.
Motor Control Exercise: Rebuild Your Core Foundation
This protocol systematically reactivates deep stabilizing muscles like your transverse abdominis and multifidus. Phase 1 focuses on isolated activation—learning to engage these muscles while breathing normally in lying or sitting positions. Phase 2 integrates limb movements while maintaining core stability during functional tasks like lifting groceries. By Phase 3, you’ll progress to loaded exercises tailored to your work or sports demands. Unlike generic crunches, this approach targets the neuromuscular control deficits fueling chronic pain, with studies showing large pain reduction effects when performed consistently.
Directional Preference Therapy: Find Your Pain-Relieving Motion
The McKenzie method identifies whether specific movements—like repeated standing back bends or prone press-ups—reduce your pain intensity or radiation. If extension movements centralize leg pain, your therapist will prescribe backward-bending exercises and extension-biased postures during daily activities. This approach delivers moderate effectiveness when a clear directional preference exists, often providing immediate relief during assessment. Key visual cues include reduced pain radiation toward your spine and improved spinal mobility after repeated motions—signs you’ve found your therapeutic direction.
Walking Protocols That Outperform Gym Routines
Simple walking programs match structured exercise effectiveness for many patients when properly implemented. Start with just 10-15 minutes daily at a comfortable pace, tracking steps rather than time. Aim for 6,000-8,000 daily steps initially, building gradually from your baseline. The critical factor? Consistency over intensity—research shows patients maintaining 5+ walking days weekly achieve better long-term outcomes than those doing sporadic vigorous exercise. Add progression by incorporating hills or intervals after 4 weeks, but never push through sharp pain increases.
Medication Strategies That Support Active Healing

Pharmacologic options should enhance—not replace—movement-based back pain therapy, with strict safety protocols.
Duloxetine: Optimizing Your Dosing Schedule
Begin with 30 mg daily for one week to minimize initial side effects before advancing to the target 60 mg dose. Track pain scores weekly on a 0-10 scale and functional improvements in daily tasks like tying shoes or rising from chairs. If you achieve less than 30% pain reduction after 4-6 weeks, discuss alternatives with your doctor—this medication isn’t effective for all pain types. Crucially, never stop abruptly; taper under medical supervision to avoid withdrawal symptoms.
NSAID Safety: Short-Term Relief Without Long-Term Damage
Use over-the-counter ibuprofen or naproxen strictly for flare-ups—never as daily maintenance. Limit continuous use to 3 weeks maximum at the lowest effective dose (e.g., 400mg ibuprofen every 8 hours). Stop immediately if you notice black stools, reduced urination, or ankle swelling—warning signs of gastrointestinal or kidney damage. Pair NSAIDs with stomach-protecting alternatives like heat therapy or acetaminophen for safer pain management.
Personalizing Your Back Pain Therapy Plan
The BACPAC precision framework matches treatments to your unique profile through structured assessment.
Your First Appointment Must Cover These 5 Areas
- Pain intensity ratings on a 0-10 scale during key movements
- Functional goals (e.g., “play with grandchildren without pain”)
- Red flag screening for serious conditions
- Depression/anxiety questionnaires
- History of previous treatment responses
Bring a 7-day pain diary tracking activities that worsen or ease symptoms—this data guides precise therapy selection. During reassessment at 4-6 weeks, expect objective measurements using tools like the ODI scale where a 10-point reduction signifies meaningful improvement.
When to Pivot Your Treatment Approach
- Less than 30% pain reduction? Switch to a different first-line therapy
- Partial response with functional gains? Add a complementary approach like ACT
- Good results at 6 weeks? Progress exercise intensity while tapering medication
- New neurological symptoms? Seek immediate imaging evaluation
Critical Safety Protocols for Home Therapy
Stop exercising immediately if you experience leg numbness, bowel/bladder changes, or progressive weakness—these indicate potential nerve compression requiring urgent care. During medication use, monitor for duloxetine-related mood shifts or NSAID-induced swelling. For self-directed programs, start at 50% intensity and prioritize pain-free ranges over aggressive stretching. The golden rule? Temporary muscle soreness is normal; sharp or radiating pain means stop.
Your 3-Month Maintenance Blueprint
Successful back pain therapy transitions from pain reduction to resilience building. Perform strength training 3x weekly (focusing on glutes and deep core), add 20-minute aerobic sessions 5x weekly, and integrate posture resets hourly during desk work. Sleep on your side with a pillow between knees and use a medium-firm mattress. When flares hit, reduce activity intensity by 50% for 3 days while applying heat—not ice—to soothe muscle tension. Track your ODI score monthly; stability above 20 points indicates robust recovery.
Final Action Steps
Don’t waste months on ineffective treatments. Start today with one evidence-based back pain therapy option matching your lifestyle: classification-based exercise if you prefer movement, duloxetine if medication suits you, or a digital program for flexible self-management. Track your pain scores and functional wins weekly—this data is your compass for adjustments. Within 6-12 weeks of consistent effort, most patients achieve significant functional gains. Your next critical move? Schedule an evaluation with a provider trained in classification-based assessment, armed with your pain diary and specific functional goals. Relief isn’t about a single magic solution—it’s about strategically combining proven therapies tailored to your body’s needs.