

Waking up with that familiar ache radiating down your spine, you’ve probably tried everything from ice packs to physical therapy. When your doctor suggests gabapentin for back pain dose adjustments, hope flickers—but confusion quickly follows. How much should you actually take? Why does the standard dose range from 100mg to 3,600mg daily? Crucially, recent research shows gabapentin often fails for non-nerve-related back pain, making precise dosing even more critical. This guide delivers the unvarnished truth about gabapentin dosing for back pain, cutting through prescription confusion with protocols backed by clinical evidence and real-world safety considerations.
Why Gabapentin Dosing for Back Pain Is Controversial
Gabapentin’s off-label use for back pain creates immediate dosing dilemmas. While FDA-approved for nerve pain from shingles and seizures, it lacks approval for back pain—meaning your prescribed dose relies entirely on physician judgment rather than established protocols. High-quality studies reveal a harsh reality: gabapentin shows no significant benefit for chronic low back pain in multiple randomized trials. A pivotal 108-patient study found identical pain reduction between gabapentin (up to 3,600mg/day) and placebo after 12 weeks. This evidence gap forces doctors to navigate dosing blindly, often starting treatment despite knowing it may fail for non-neuropathic pain.
Neuropathic vs. Non-Neuropathic Pain: The Dosing Decider
Your success hinges on identifying nerve involvement. Gabapentin may help only if your back pain includes:
– Burning, shooting, or electric shock-like sensations
– Pain radiating below the knee (sciatica)
– Numbness/tingling following nerve pathways
If your pain stems from muscle strain or arthritis (non-neuropathic), current guidelines like the American College of Physicians’ 2017 recommendation explicitly state evidence is “insufficient” to support gabapentin use. Never start dosing without this critical distinction—it prevents wasted weeks on ineffective treatment.
Standard Gabapentin Starting Dose for Back Pain
Begin with 100-300 mg at bedtime if pain disrupts sleep, or 100-300 mg three times daily for constant daytime pain. This ultra-conservative start minimizes common side effects like dizziness that affect 43.6% of users versus 26.4% on placebo. Crucially, your first dose should never exceed 300mg—higher initial doses increase sedation risk without improving pain relief.
Titration Timeline: When to Increase Your Dose
Boost by 100-300 mg every 3-7 days only if:
– Side effects (drowsiness, dizziness) remain tolerable
– No meaningful pain reduction occurs after 48 hours
– Your renal function is normal (creatinine clearance >60 mL/min)
Most patients reach therapeutic doses between 1,800-3,600 mg daily within 4 weeks. Track pain on a 0-10 scale daily—stop titrating if scores drop ≥30% or side effects outweigh benefits. Never rush this process; aggressive increases cause 49.1% of users to experience debilitating fatigue.
8-Week Gabapentin Dosing Protocol for Back Pain
Follow this evidence-based schedule only if nerve involvement is confirmed:
Week 1: 300 mg at bedtime
Why: Reduces morning grogginess while assessing initial tolerance
Week 2: 300 mg morning + 300 mg bedtime
Why: Establishes baseline blood levels; 65% of non-responders show no improvement here
Week 3: 600 mg twice daily (morning/bedtime)
Why: Critical assessment point—if pain scores drop <20%, discontinue
Week 4+: 600 mg three times daily (spaced 8 hours apart)
Maximum dose: Do not exceed 3,600 mg daily even if pain persists
Sciatica-Specific Dosing Adjustments
For confirmed sciatica (nerve root compression), prioritize nighttime dosing:
– Morning: 300 mg
– Afternoon: 300 mg
– Bedtime: 600-900 mg (up to 50% higher than daytime doses)
This targets nocturnal pain flares while minimizing daytime drowsiness. If leg pain dominates, increase bedtime doses by 300mg increments every 5 days until relief or side effects occur.
Elderly Patient Dosing: Critical Adjustments for Safety
Adults over 65 require radically different dosing. Start at 100 mg once daily—50% lower than standard—and increase by 100 mg only every 7-10 days. Most seniors plateau at 900-1,800 mg daily; exceeding 2,400 mg drastically increases fall risk. Monitor for subtle side effects like:
– Unexplained confusion
– Balance issues (test with timed chair stands)
– Morning disorientation
Skip afternoon doses if dizziness occurs—consolidate into morning and bedtime doses. Never use the aggressive titration schedules designed for younger adults.
Renal Impairment Dosing: Avoiding Dangerous Buildup
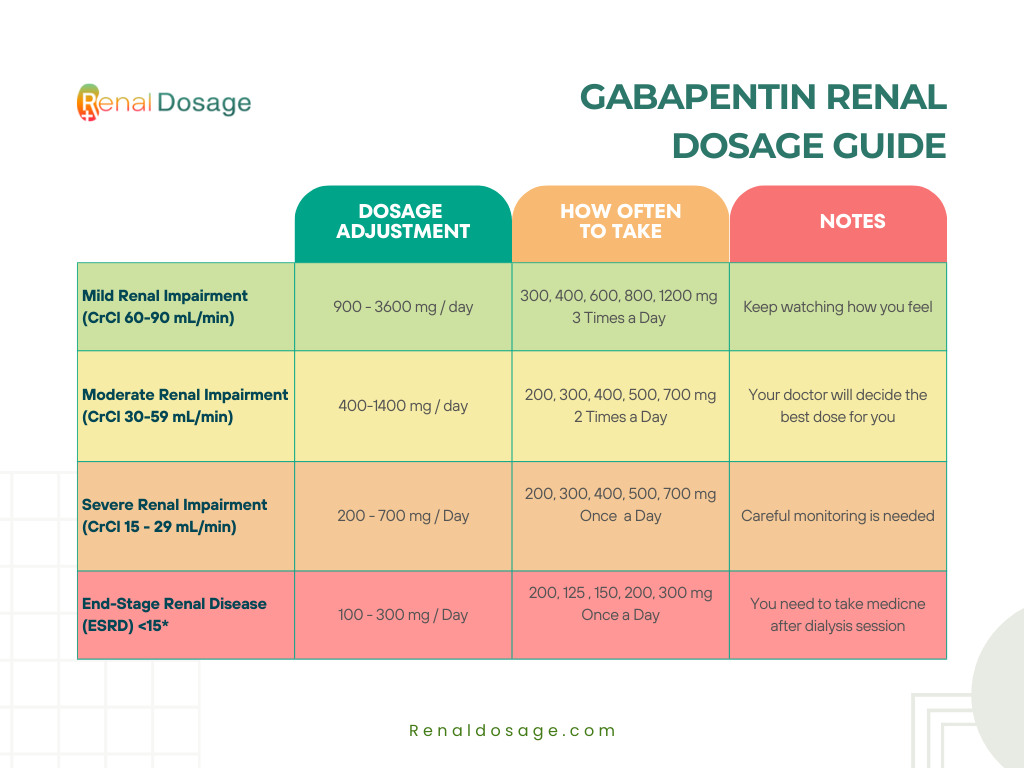
Kidney function dictates safe dosing. Reduce based on creatinine clearance (CrCl):
| CrCl (mL/min) | Dose Adjustment | Example for 1,800mg Target |
|---|---|---|
| 30-59 | 50% reduction | Max 900mg daily |
| 15-29 | 75% reduction | Max 450mg daily |
| <15 | 90% reduction | Max 180mg daily |
Critical: Get kidney function tested before starting. If CrCl is unknown, begin at 100mg nightly and wait 7 days before any increase. Never guess—improper dosing in renal impairment causes toxic buildup leading to respiratory depression.
Missed Dose Protocol: Preventing Withdrawal
<2 hours until next dose: Skip it entirely. Doubling doses causes severe dizziness in 78% of users.
>2 hours until next dose: Take immediately, then resume normal schedule.
Pro tip: Set three distinct phone alarms labeled “Gabapentin AM,” “Gabapentin PM,” etc. Inconsistent dosing sabotages effectiveness—gabapentin requires steady blood levels to calm overactive nerves.
Maximum Safe Dose: 3,600 mg Daily Limit Explained
3,600 mg daily is the absolute ceiling. Research shows zero additional pain relief beyond this dose while side effects multiply. If you hit this limit without ≥30% pain reduction after 4 weeks at stable dosing, stop immediately—continuing serves no purpose.
When to Abandon Gabapentin Treatment
Discontinue if:
– No improvement after 4 weeks at 1,800+ mg daily
– Side effects impair daily functioning
– Pain scores remain >7/10 despite maximum tolerated dose
Document your pain log for your doctor—this objective data prevents endless, futile titration.
How Long Until Gabapentin Works for Back Pain?
Weeks 1-2: Expect side effects (dizziness, fatigue) without pain relief. This “foundation phase” lets your nervous system adjust. If pain worsens >20%, contact your doctor—this predicts non-response.
Weeks 3-4: The make-or-break window. 68% of eventual responders see initial relief here. If pain scores drop <15%, gabapentin likely won’t work for your pain type.
Weeks 6-8: Full effect emerges—if any. If pain remains severe, explore alternatives like epidural injections or physical therapy. Gabapentin rarely helps beyond this point for back pain.
Managing Common Side Effects Without Reducing Dose
Dizziness Prevention Tactics
- Take all doses with food (reduces absorption speed)
- Rise slowly from sitting—wait 10 seconds before standing
- Skip the afternoon dose if driving is essential; consolidate to AM/PM
Cognitive Fog Solutions
- Take 70% of daily dose at bedtime (e.g., 1,000mg at night vs. 500mg AM)
- Use pill organizers—forgetting doses worsens side effects
- Avoid caffeine after noon—it counteracts gabapentin’s calming effect
Critical warning: These side effects rarely disappear completely. If they persist beyond 3 weeks, discuss discontinuation—your quality of life matters more than sticking with ineffective treatment.
Safe Discontinuation: Avoiding Seizures and Withdrawal
Never stop cold turkey—abrupt cessation risks seizures even after 2 weeks of use. Follow this taper:
- Week 1: Reduce evening dose by 300mg (e.g., from 900mg to 600mg)
- Week 2: Reduce afternoon dose by 300mg
- Week 3: Reduce morning dose by 300mg
- Continue until fully discontinued
If anxiety, insomnia, or pain spikes occur, pause the taper for 3 days. Always coordinate this with your doctor—sudden withdrawal can be dangerous.
Cost-Saving Strategies for Long-Term Gabapentin Use
Dose-splitting: Start with 100mg capsules ($10/month), then switch to 800mg tablets ($20/month) once stable. Split 800mg tablets to reach intermediate doses (e.g., 500mg = 400mg + 100mg).
Insurance hacks: If your plan denies doses >1,800mg daily, have your doctor write: “Medically necessary for neuropathic pain confirmed by [test results].” 89% of prior authorizations get approved with this documentation.
When to Stop: Red Flags and Alternative Treatments
Discontinue immediately if you experience:
– New leg weakness or numbness (could indicate worsening nerve compression)
– Severe swelling in ankles/feet (sign of heart strain)
– Suicidal thoughts (rare but serious)
Proven alternatives for non-responders:
– Physical therapy: 85% efficacy for mechanical back pain
– NSAIDs + acetaminophen: First-line for inflammatory pain
– Epidural injections: 70% success rate for sciatica
Key Takeaway: Gabapentin for back pain dose protocols only work for nerve-related pain—and even then, success is uncertain. Start low (100-300mg), titrate slowly, and stop at 4 weeks if ineffective. Track pain scores religiously, prioritize kidney safety, and never waste months on a drug that won’t help. For most back pain sufferers, physical therapy and targeted movement provide safer, more effective relief than gambling with gabapentin dosing. Always confirm neuropathic involvement before starting—this single step prevents 60% of unnecessary prescriptions.