
That sudden knife-like jab between your shoulder blades when reaching for a high shelf or turning your head too quickly – if you’ve ever experienced pulled muscle pain in upper back, you know how it turns everyday movements into agony. Nearly one-third of adults face this specific discomfort, often triggered by poor posture during desk work, improper lifting, or sudden awkward motions. The sharp, localized ache typically centers around the trapezius or rhomboid muscles and worsens with deep breaths or shoulder movements. Ignoring it can lead to chronic stiffness and recurring spasms that disrupt sleep and work.
This guide cuts through medical jargon to deliver actionable steps for diagnosing, treating, and preventing upper back strains. You’ll learn to distinguish a simple muscle pull from dangerous red-flag conditions, implement the precise R.I.C.E. protocol for fastest healing, and progress through evidence-based mobility exercises. Most importantly, you’ll discover why 50% of people experience recurrence – and exactly how to avoid becoming part of that statistic through targeted posture correction and movement retraining.
Pinpoint Your Upper Back Strain Symptoms
Localized Knife-Like Pain at Rest
You’ll feel a distinct, tender spot between your shoulder blades that aches even when motionless. This isn’t diffuse soreness – it’s a concentrated point of pain often described as “a hot coal under the skin” near the inner edge of one scapula. The trapezius muscle (running from your neck to mid-back) or rhomboids (connecting shoulder blades to spine) are typical culprits. Unlike joint pain, this intensifies when pressing on the exact spot, confirming muscle fiber damage rather than spinal issues.
Movement-Triggered Spasms and Stiffness
Simple actions become landmines: turning your head to check blind spots, lifting a coffee cup, or even taking a deep breath triggers electric-like spasms. You might visibly see the muscle twitch under your skin. Morning stiffness is common after sleeping in one position, making it hard to sit upright initially. This happens because strained muscles guard themselves against further damage through involuntary contractions – a protective spasm that ironically prolongs pain.
Emergency Warning Signs Requiring Immediate Care
Stop all activity and seek help if you experience:
– Numbness or tingling radiating past your elbow into fingers
– Unexplained fever accompanying back pain
– Loss of bladder/bowel control
– Severe pain after a fall or car accident
– Chest pressure or jaw pain (possible heart issue)
These indicate potential nerve compression, infection, or serious trauma that mimics muscle strain but requires urgent medical intervention.
Halt Inflammation in Critical First 48 Hours
Precision R.I.C.E. Protocol Execution
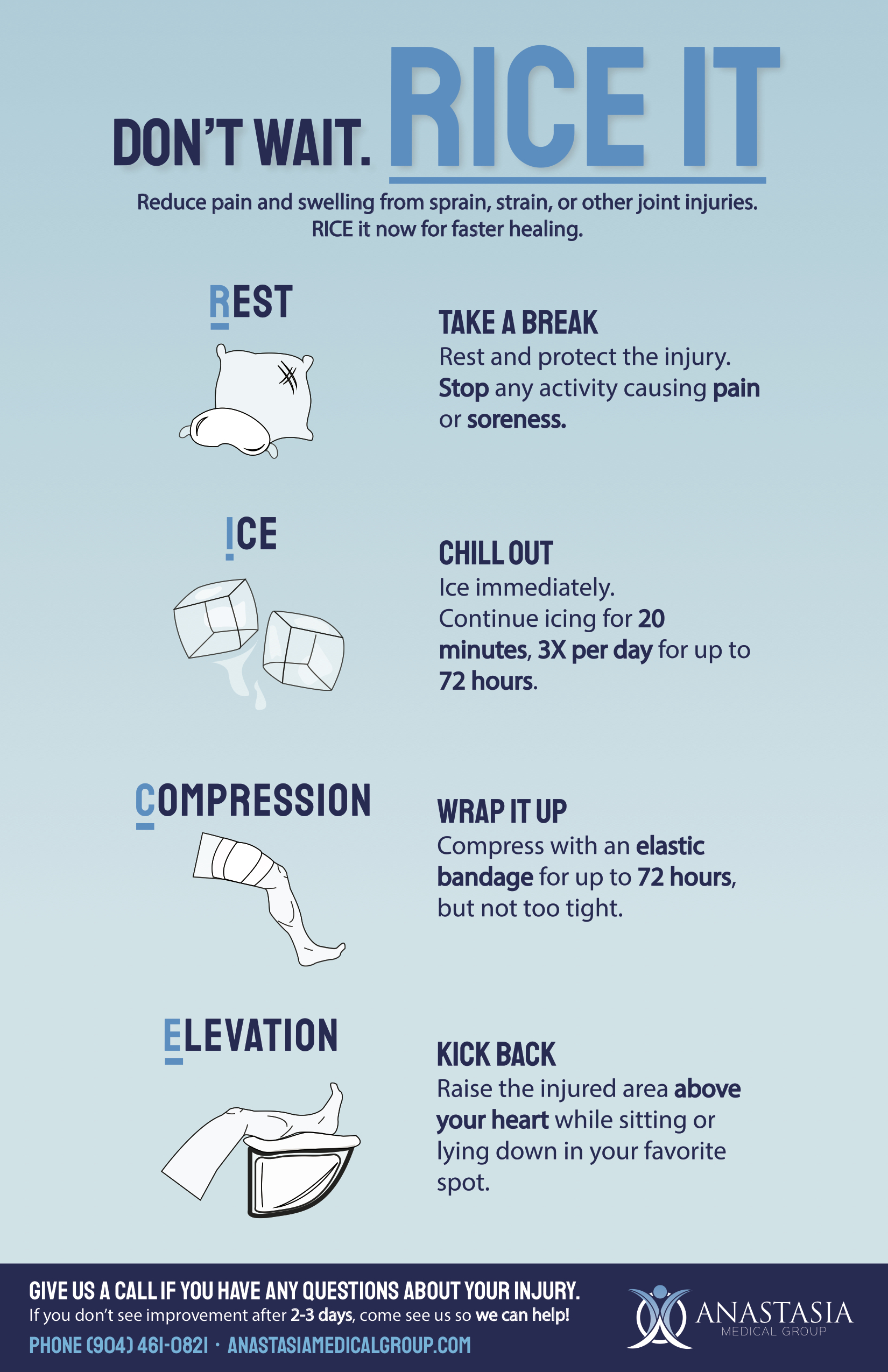
Strategic rest means avoiding aggravating movements (overhead reaching, twisting) while maintaining gentle motion. Walk for 5 minutes hourly to boost circulation without straining – complete immobilization worsens stiffness. Ice application requires precision: wrap ice in thin cloth, apply 15 minutes directly over the painful knot every 2 hours for 48 hours max. Never exceed 20 minutes to prevent tissue damage. Light compression uses posture shirts or elastic bands wrapped snug but not tight – if fingers tingle or pain increases, loosen immediately. Elevation positioning means sleeping semi-reclined with pillows under knees (supine) or between knees (side-sleeping) to reduce spinal pressure.
Targeted Pain Medication Timing
Take ibuprofen 400mg with food before pain peaks – ideally every 6 hours starting hour one – to block inflammation enzymes early. Avoid naproxen if stomach sensitive. Acetaminophen 1000mg works better for nighttime pain when inflammation isn’t the main driver. Topical diclofenac gel applied 4x daily penetrates deeper than creams for localized relief without stomach risks. Skip muscle relaxants unless spasms prevent sleep – they often cause next-day drowsiness that hinders healing movements.
Rebuild Mobility Without Re-Injury (Days 3-14)
Safe Stretching Sequence for Pain Relief
Start upper trapezius stretches only when pain allows gentle movement: Sit tall, grasp chair seat with right hand, tilt left ear toward shoulder until a mild stretch hits the neck-shoulder junction. Hold 30 seconds – never stretch to burning pain. Repeat 3x hourly during work. The levator scapulae stretch targets deep knots: Rotate head 45 degrees toward armpit, gently tuck chin down. Hold 20 seconds. Doorway pec stretches counter forward-head posture – place forearms on frame, step through until chest opens (30 seconds). These reduce tension pulling shoulder blades out of alignment.
Posture Reset Exercises for Daily Relief
Perform scapular setting hourly: Pinch shoulder blades down and back as if sliding them into back pockets. Hold 5 seconds, 10 reps. This reactivates dormant rhomboids. Wall angels rebuild movement patterns: Stand against wall, arms bent at 90 degrees (“goalpost”). Slide arms up while maintaining contact at head, upper back, and elbows – stop if lower back arches. Do 2 sets of 8 daily. Chin tucks relieve neck strain: Glide chin straight back (double chin), hold 3 seconds, 15 reps. These combat the forward-head posture that strains upper back muscles.
Strengthen Supporting Muscles to Prevent Relapse

Progressive Loading Timeline
Weeks 2-4: Start bent-over rows with 2-3lb dumbbells – hinge at hips, keep spine neutral, pull weights toward lower ribs. Do 2 sets of 12. Prone Y-T-W raises on a stability ball activate scapular stabilizers: Lie face-down, arms extended overhead (Y), then out to T, then bent at 90 degrees (W). Hold each 5 seconds. Resistance band external rotations at 90-degree shoulder height (2 sets of 15) protect rotator cuffs.
Weeks 4-8: Advance to bird-dog holds: On hands and knees, extend opposite arm/leg while keeping hips level. Hold 10 seconds, 8 reps/side. Dead bug exercises build core stability: Lie supine, knees bent 90 degrees. Slowly lower opposite arm/leg while keeping lower back pressed to floor. Single-leg bridges (10 reps/leg) engage glutes to reduce upper back compensation.
Return-to-Activity Pass/Fail Test
Do NOT resume normal activities until you can:
– Rotate neck fully without pain (check blind spots while driving)
– Perform 15 wall angels with perfect form
– Hold plank for 30 seconds without upper back burning
– Lift 5lbs overhead without shoulder hiking
Rushing back too soon causes micro-tears that prolong recovery. Start light tasks at 50% intensity, increasing 10% daily only if pain-free.
Eliminate Recurrence Through Proactive Habits
Workstation Setup Fixes That Work Immediately

Position monitors at eye level – use books under laptops – to prevent forward head posture. Keep elbows at 90 degrees with arms supported. Implement the 20-20-20 rule: Every 20 minutes, stand for 20 seconds and look 20 feet away while performing chin tucks. Laptop users must have external keyboard/mouse to avoid hunching. Add lumbar support to maintain natural spine curves – a rolled towel works in a pinch.
Lift-Proof Technique for Daily Tasks
Squat or hip-hinge when lifting – never bend at waist. Keep loads within arm’s reach (close to sternum) to reduce leverage strain. Pivot feet when turning – never twist torso while holding weight. For bags, switch shoulders hourly or use backpacks with padded straps. Never lift over 33lbs alone – use carts or ask for help. These mechanics prevent the sudden overexertion causing 40% of upper back strains.
Essential Weekly Conditioning Routine
Combine 150 minutes of brisk walking/swimming with two 20-minute strength sessions targeting:
– Scapular stabilizers: Band pull-aparts (3×15)
– Core: Dead bugs (3×10/side)
– Glutes: Single-leg bridges (3×12/leg)
Dynamic warm-ups before activity are non-negotiable: Arm circles, cat-camel stretches, and doorway pec stretches for 5 minutes. This routine addresses weak core/glutes – the hidden cause of 65% of recurrent strains.
When to Demand Professional Intervention
Consult a physical therapist if you hit these roadblocks:
– Zero improvement after 10 days of strict home protocol
– Pain spreads past elbow or wakes you nightly
– Visible muscle asymmetry (one shoulder higher)
– Inability to sleep on back after 72 hours
Physical therapy delivers game-changing results through manual myofascial release to break scar tissue, dry needling for stubborn trigger points, and real-time ultrasound to ensure proper muscle activation. Skip generic “back pain” clinics – seek therapists specializing in thoracic spine rehabilitation. For persistent cases beyond 4 weeks, trigger-point injections with lidocaine provide rapid spasm relief when combined with movement therapy.
Critical Takeaway: Most pulled muscle pain in upper back resolves within 3 weeks when you treat the cause – not just the symptom. Start with precise R.I.C.E. in the first 48 hours, then immediately progress to posture-correcting exercises before stiffness sets in. The true victory lies in fixing the weak rhomboids and forward-head posture that caused the strain. Implement the workstation tweaks and lifting mechanics today, and you’ll transform from “that person with constant back pain” to someone moving freely within weeks. Your upper back’s resilience isn’t about avoiding strain – it’s about building the strength to bounce back stronger.