

That stabbing sensation at the back of your heel isn’t just annoying—it’s a red flag your body is waving. Sharp heel pain can stop you from walking comfortably, ruin your favorite shoes, and turn simple activities into daily torture. But here’s what most people don’t realize: the size of the problem rarely matches the intensity of your pain, making proper diagnosis absolutely critical.
Whether you’re dealing with bone spurs, inflamed bursa, or biomechanical issues, this guide walks you through everything you need to know about posterior heel pain—from identifying the exact cause to understanding your treatment options.
Pinpoint Your Exact Heel Pain Cause
Sharp Pain vs. Dull Ache Patterns
When you experience sharp pain on heel back, the quality of your pain provides crucial diagnostic clues. Sharp, knife-like sensations typically indicate bone-related issues such as exostosis or Haglund deformity, while burning or aching points toward soft tissue problems like bursitis. Your pain pattern—whether it strikes during activity or after resting—helps distinguish between these conditions. Bone-related pain often worsens with shoe pressure, while soft tissue inflammation may feel warm and swollen to the touch.
Common Pain Triggers to Track
Identify your specific triggers by noting when your heel pain intensifies. Morning first steps causing severe pain that eases with movement suggest plantar fasciitis rather than posterior issues. Pain increasing with rigid heel counters points directly to Haglund deformity. Activity-onset pain developing during exercise (not after) indicates bone spur irritation. Rest relief where pain decreases when you stop moving often accompanies Achilles tendon involvement. These patterns help your podiatrist determine if your sharp pain on heel back stems from bone growth, bursa inflammation, or biomechanical problems.
Three Main Causes of Posterior Heel Pain

Bone Growth in Achilles (Exostosis)
This progressive condition involves actual bone formation within your Achilles tendon, creating a hard, painful lump at the back of your heel. Overuse and chronic tendon pulling trigger this problem that worsens over months or years. The pain feels like a knife in your heel, especially when wearing shoes, as the bone growth rubs against surrounding tissues. Unlike other heel conditions, exostosis continues developing over time without intervention, eventually requiring surgical removal when conservative treatments fail.
Haglund Deformity (Bony Bump)
Characterized by a prominent bony protrusion on your heel’s back, this deformity often pairs with a high-angled heel bone. The bump irritates surrounding tissues, creating a painful cycle of inflammation and tissue damage. You’ll notice a visible bump that rubs against every shoe you wear, causing redness and swelling. Haglund deformity frequently develops in people with high arches or rigid foot structure, and while it may not cause pain initially, the constant shoe friction eventually leads to sharp pain on heel back that worsens with activity.
Inflamed Bursa (Retrocalcaneal)
The fluid-filled pocket behind your heel, designed to reduce friction, becomes swollen and painful. This rarely occurs alone—usually accompanying bony abnormalities like Haglund deformity. The pain feels like pressure and warmth, often with visible swelling around your Achilles tendon insertion point. Unlike bone-related pain that feels sharp with pressure, bursitis creates a diffuse ache that may radiate up your calf. You’ll notice increased pain when you press on the back of your heel or wear shoes with stiff heel counters.
Conservative Treatment Options That Work
Early-Stage Management
Starting conservative care early improves your chances of avoiding surgery for sharp pain on heel back. Your podiatrist will tailor non-surgical treatments to your specific diagnosis, focusing on reducing pain and preventing progression. While studies show limited long-term success for severe cases, many patients find significant relief with proper footwear modifications and activity adjustments. The key is identifying your specific pain trigger and addressing it before inflammation becomes chronic.
Effective Non-Surgical Interventions
- Footwear modifications: Switch immediately to shoes with soft heel counters that won’t aggravate your heel bump
- Orthotic devices: Custom inserts redistribute pressure away from your painful area
- Activity modification: Reduce impact activities temporarily while maintaining fitness
- Anti-inflammatory measures: Ice therapy 3-4 times daily and NSAIDs as directed
- Stretching routines: Gentle Achilles and calf stretches prevent tightness that worsens pain
Surgical Solutions When Conservative Care Fails
Bone Spur Removal (45-Minute Procedure)
This procedure removes bone growth from the back of your heel, including any pieces extending into your Achilles tendon. The surgeon reattaches your Achilles using anchor sutures—special bone-anchored stitches that hold everything in place. Recovery requires a cast to knee level with full healing taking up to one year. Persistent pain may occur if your Achilles tendon quality is poor, highlighting why proper diagnosis matters before surgery.
Haglund Bump Correction

Your surgeon makes a 6 cm incision near the Achilles tendon, removes the bony prominence, and reattaches the tendon. Unlike spur removal, this focuses specifically on the prominent bump. Recovery differs significantly—you’ll wear an Aircast walker instead of a full cast, which you can remove during rest periods. This approach typically offers faster initial recovery than traditional spur removal procedures.
Day Surgery Process Demystified
Pre-Operative Steps
Your same-day admission includes changing into a surgical gown, confirming consent, and marking the surgical site. The anesthesiologist reviews your medical history while nurses prepare you for the procedure. Full disclosure of your health history during this phase helps minimize risks—don’t skip mentioning medications or previous complications.
Anesthesia Options
Most patients receive both general anesthesia and a popliteal block (local anesthetic behind your knee using nerve stimulator guidance). This combination provides 24-36 hours of pain and movement blockage, making your first days of recovery significantly more comfortable. The nerve block wears off gradually, preventing sudden pain spikes when it subsides.
Recovery Timeline and Milestones
First 48 Hours Critical Period
Elevate your leg continuously and use crutches only when absolutely necessary. Keep your cast or dressing completely dry—waterproof covers help with bathing. Arrange for 24-hour supervision and transportation home. This initial period sets the stage for successful healing, so strict adherence to instructions matters most now.
Week-by-Week Progression
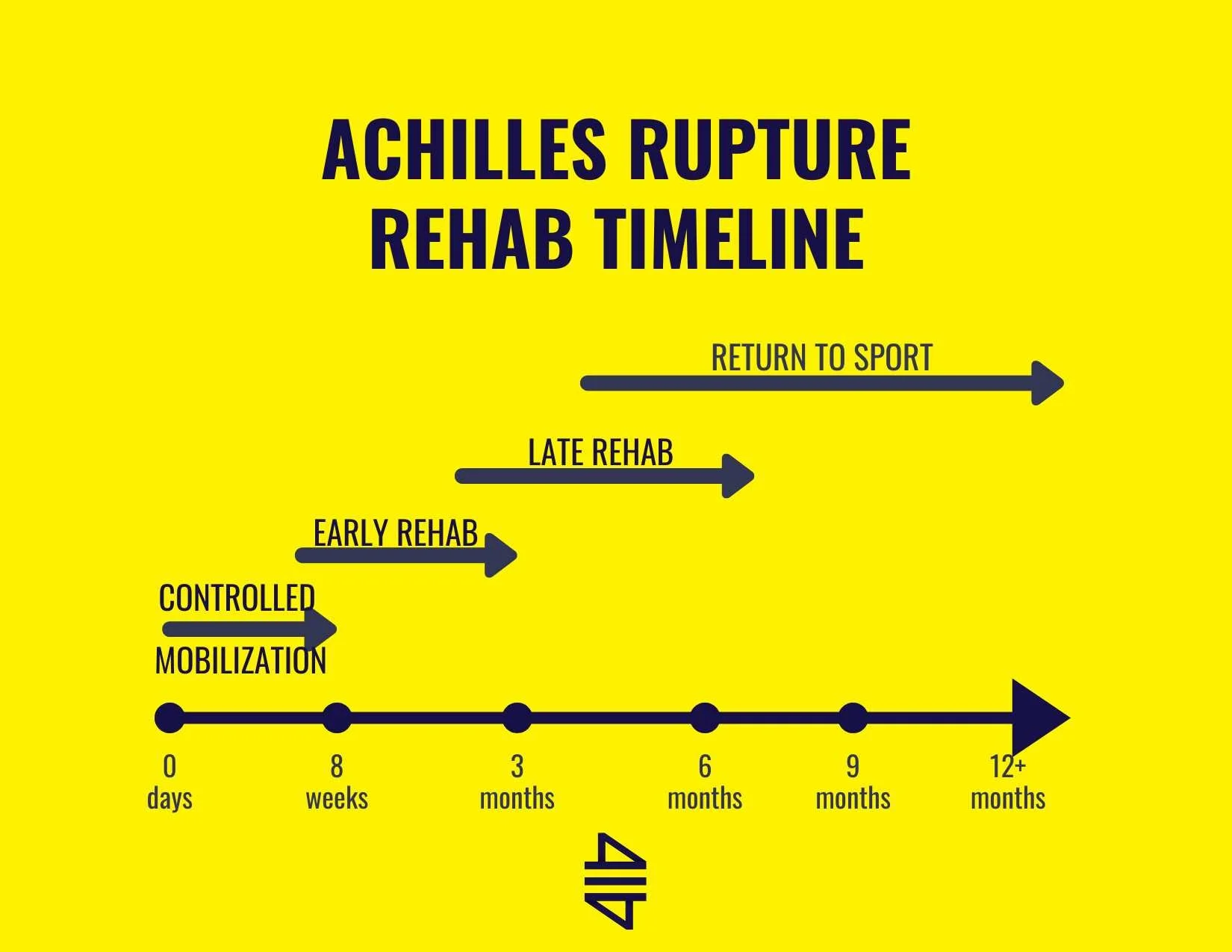
Your recovery follows a predictable pattern: Weeks 1-2 require complete non-weight bearing; Weeks 3-6 introduce gradual weight-bearing; Weeks 6-12 begin physical therapy; Months 3-6 allow return to normal activities; Months 6-12 bring full strength and function return. Individual variation exists, but skipping stages risks complications that prolong healing.
DVT Prevention Protocol You Must Follow
Risk Factors and Prevention
Being in a cast and non-weight bearing significantly increases blood clot risk. You’ll self-inject low molecular weight heparin into your abdomen throughout the non-weight bearing period. Rotate injection sites to prevent bruising—this simple step prevents painful complications that could sideline your recovery.
Daily Prevention Routine
Inject at the same time each day using proper subcutaneous technique in your abdomen. Continue throughout your cast/non-weight bearing period as directed, storing medication refrigerated as required. This routine prevents potentially life-threatening blood clots while you heal from surgery for your sharp pain on heel back.
Complication Prevention Strategies
Pre-Surgical Optimization
Full medical history disclosure enables your surgical team to identify and minimize risks. Multi-disciplinary consultation happens when health queries arise, ensuring optimal surgical outcomes. Disclose all medications, especially blood thinners, to prevent bleeding complications during your heel surgery.
Lifestyle Modifications
Stop smoking at least four weeks before surgery—smokers face 20% increased delayed healing risk. Restrict alcohol to prevent drug interactions and healing impairment. Focus on nutrition with protein-rich foods to support tissue healing. Follow prescribed mobilization routines precisely—these seemingly small steps dramatically impact your recovery success.
When to Seek Professional Help Immediately
Red Flag Symptoms
Contact your surgeon immediately if you experience severe pain uncontrolled by medication, numbness or tingling in your foot, signs of infection (fever, chills, wound drainage), or cast problems (too tight, broken, or wet). These warning signs indicate potential complications requiring urgent attention to prevent permanent damage.
Long-Term Success Factors
Individual recovery varies significantly, but patient compliance remains the strongest predictor of success. Follow your surgeon’s instructions precisely, attend all follow-up appointments, and complete prescribed physical therapy for optimal outcomes. Your active participation in recovery directly determines whether your sharp pain on heel back resolves completely or becomes a chronic issue.
Key Takeaways for Heel Pain Relief
Sharp pain on the back of your heel demands professional evaluation—self-diagnosis often leads to delayed treatment and worse outcomes. Conservative measures may suffice for early cases, but surgical intervention becomes necessary when symptoms persist or worsen. Recovery takes patience, with full healing requiring up to one year for complex procedures. Your next step: Schedule a consultation with a podiatric surgeon experienced in posterior heel conditions. Bring detailed notes about your pain patterns, footwear difficulties, and activity limitations to help guide treatment decisions. Don’t ignore that sharp pain on heel back—addressing it properly now prevents years of unnecessary suffering.